The Medical Expenditures Panel Survey (MEPS) released its latest data from 2022 last month. The MEPS is a set of large-scale government surveys that are “the most complete source of data on the cost and use of health care and health insurance coverage.” The data show that immigrants accounted for 19 percent fewer Medicaid and Medicare expenditures per capita than the US-born population from 2002 to 2022.
The MEPS “collects data on the specific health services that Americans use, how frequently they use them, the cost of these services and how they are paid for, as well as data on the cost, scope, and breadth of health insurance held by and available to U.S. workers.” The MEPS supplements its findings with data directly from medical providers so it is not based solely on people’s recollections. A key feature of the survey is that it reports the actual dollar amounts spent by birthplace, which no other survey does.
Immigrant Medicare and Medicaid Costs
Figure 1 shows the total inflation-adjusted per capita Medicare and Medicaid expenditures for 2002 to 2022. The data exclude the years 2004 to 2006, when no birthplace variable was included, and 2013, when a survey weighting issue prevented using the birthplace variable. In 2022 dollars, foreign-born people (mainly immigrants, plus some children of Americans born abroad) received $1,775 per person, compared to $2,180 per person for US-born individuals. Immigrants accounted for 19 percent less government Medicare and Medicaid spending than US-born individuals.
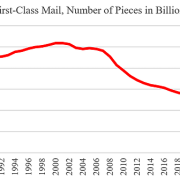
Figure 2 shows that this pattern of lower spending has persisted for the last 20 years. For the available years, immigrants accounted for 11.5 percent of combined Medicare and Medicaid spending. Cumulatively, if the average immigrant had cost as much as the US-born population, the government would have had to spend about $300 billion more in those years. The full data are displayed in Table A at the end of this post.
The MEPS data has an interesting effect on estimates of the fiscal consequences of immigration. In its 2017 study, the National Academies of Sciences, Engineering, and Mathematics (NAS) used a two-step process to estimate Medicare and Medicaid spending costs, which Cato used in its 2023 report. First, the NAS used the Current Population Survey Annual Social and Economic Supplement to find the number of immigrants enrolled in those programs and then used the National Health Expenditure Accounts (NHEA) to identify per-capita costs per enrollee by age and gender. The NHEA does not distinguish between spending by birthplace or citizenship.
Table 1 compares the distribution of spending under the NAS methodology compared to the MEPS. It updates the NAS work through 2022. The NAS model assigns about the same amount of Medicare spending to immigrants as the MEPS (9.6 percent to 10.3 percent), but the real difference emerges for Medicaid. The NAS model assigns nearly 16.7 percent of spending to immigrants, compared to the MEPS, which finds just 13.6 percent—19 percent lower. Medicaid is a smaller program, but as it is means-tested, it disproportionately affects the estimates among low-wage immigrants.
Why Immigrants Use Less Medicare and Medicaid
Despite their lower incomes, immigrants are less likely to use publicly funded health care for several reasons. Most importantly, they are younger, but even controlling for age, immigrants tend to be healthier and participate in fewer high-risk activities. In addition, their eligibility for Medicare and Medicaid is more limited than for the US-born population. They need to be lawfully present and to have worked ten quarters in the United States to qualify for Medicare. And, in most cases, they need to have lived for at least five years as a lawful permanent resident to qualify for Medicaid, where the state government pays for it. Finally, some eligible immigrants also do not enroll in these programs out of ignorance or fear about its immigration effects.
The government should go further to restrict immigrant eligibility for Medicare and Medicaid. The best experimental evidence indicates that Medicaid does not improve health outcomes for participants, and unnecessarily shifts health care costs onto taxpayers. When Congress eliminated Medicaid eligibility for many immigrants in the 1990s, the share of immigrants without health insurance did not rise. Those same immigrants increased their work effort and took jobs that offered health insurance. Reducing the taxpayer costs of immigration would increase the already substantial fiscal benefits of immigration, making positive reforms more likely.
Immigrants positively affect the health care system in the United States. Although immigrants receive benefits, they also pay taxes and premiums to cover the costs of their expenditures. As doctors, nurses, health aides, and assistants, they also directly provide services that reduce the cost of health care in the United States. These workers improve health outcomes for Americans. If members of Congress truly care about improving Americans’ health care, they should make legal immigration substantially easier.
Notes: This post expands on findings by Drishti Pillai and Samantha Artiga of the Kaiser Family Foundation that reviewed the MEPS immigrant health care spending for 2021. I appreciate them sharing their methodology. Mike Howard used Cato’s updated NAS model to calculate immigrant Medicare and Medicaid costs